
Mapping the hip joint (a biomechanics breakdown)
- Dominik Koch
- Feb 27, 2023
- 8 min read
Updated: Mar 8, 2023
Hip pain? Let's see what that's about... We will build on our map that I talked about in a previous article. I strongly suggest that you read it if you haven't already, as some of things in today's article might be difficult to understand without the foundations that I laid in that article.
What is the hip?
This might be obvious when I say it, but in order to understand our hip and a potential problem with it, we first want to be clear on what the hip actually is. The majority of people don't know this, so let's make it clear: The hip is not the pelvis. The hip is also not the side of the leg. The hip is a joint, i.e. it is a space where (in this case) two bones meet. These bones are the leg (the femur) and the pelvis (also bone). The space in-between those two bones, that is our hip joint. Highlighted in green is the pelvis, in grey is the femur. The space where these two meet: that is the hip joint (highlighted in red).
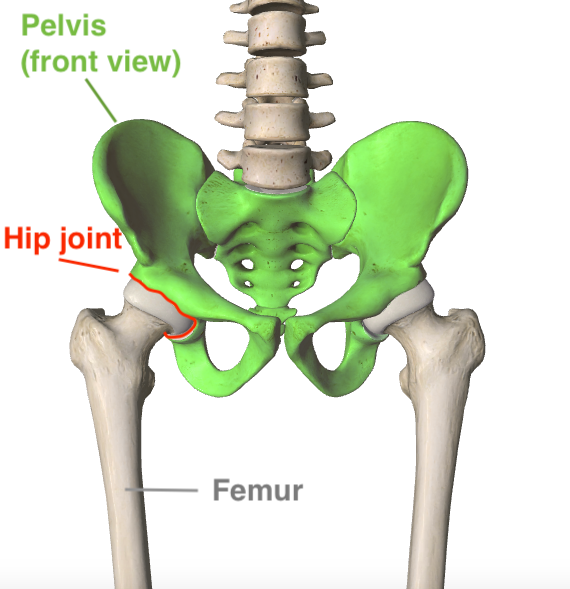 |  |  |
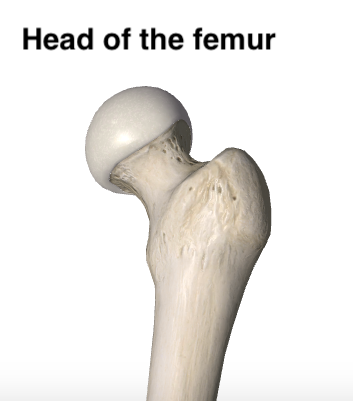
The hip joint is a "ball and socket joint", because the top of the femur (leg) is ball-shaped, whereas the cavity at the pelvis is the "socket" that this ball sits in:
 |  |
Whenever we talk about hip motion, we talk about a change in orientation between the bones, within that space. Hip motion is not the same as pelvis motion, and it's also not the same as leg motion. It is only 'hip motion' when the two move in relation to each other.
Hip muscles
If we experience problems in a muscle around the hip, we want to understand what that muscle is being put through via the motion of the underlying hip joint. There are quite a few muscles that attach to the femur and the pelvis. Therefore, if we change the orientation of these two bones (=hip motion) we create a length change in those muscles - please recall the "movement spectrum" article here .
We won't go into too much detail for each muscle individually here, but let's have a look at how many muscles there are around this region:
 |  |  |
If there is motion at the hip joint, these muscles will either lengthen or shorten.
Got a problem with a muscle around the hip? If not you, then you probably at least know someone who has complained about one of multiple of the muscles listed below.
Hamstrings
Glutes
Adductors
Piriformis + other pelvic floor muscles
Hip flexors
TFL / IT Band
What do they have in common? They are all affected by hip motion - and the lack of it!
It doesn't matter where you experience problems around the hip (even if it's in the joint itself), we just want to know what that area is going through. IF the hip can move freely in all 3 planes of motion, all of these muscles (and ligaments) will get the chance to lengthen and shorten. The joint itself gets the chance to compress and decompress. Wouldn't that be nice?!
But how to find out?
Again, with structure. We will investigate our movement at the hip according to our 3 planes of motion again. The goal is to find out where we are limited and then of course, to restore all of that freedom.
Hip motion breakdown
As before, we will investigate our sagittal plane, frontal plane and transverse plane separately, all with a view on the pelvis motions that we have already discussed in the previous article.
For each plane, we will ask ourselves the question: "in this plane of motion, is the angle at the hip opening or closing?" (Remember, surrounding muscles will be affected by that - "joints act, muscles react")
1. Sagittal plane hip motion

Recall these images from before: If we have the ability to move our pelvis around the femur, then we can create movement of hip flexion via an anterior tilt, and hip extension via a posterior tilt.
The closing of the angle at the front of the hip is called hip flexion. The opening of the angle at the front of the hip is called hip extension.
Very often, people do not have separate pelvis and leg motion and it's all glued into one big block, therefore they do not have these motions at the hip joint, and they will compensate elsewhere:
If you try these tilts yourself, check:
Do you get any compression in your lower back when you anteriorly tilt the pelvis? Rather than flexing the hip, you might be extending your spine excessively. If the hip is not moving, something else will and very often this is the back here.
Likewise, in that same anterior tilt, do you pull your legs and knees back (extend the knees)? Here as well, you are 'skipping' the hip joint and there is no, or little, pelvis to femur articulation.
When you posterior tilt, do you push your knees forward? If you do, can you see how that forward movement of the leg and knee is not really opening the angle at the front of your hip? The outcome: no hip motion.
If you have problems with your hamstrings, hip flexors or glutes (or lower back for that matter), this is important information. Write down your findings.
2. Frontal plane hip motion

Recall the frontal plane images from the map article: We can drop and hike the pelvis. Again we are now interested in the angle between the pelvis and the femur. What you can see on the image is that the side that drops opens the angle between leg and pelvis, whereas the hiking side closes. These are called hip abduction (green, opening) and hip adduction (red, closing) respectively.
When you try this (keep both feet on the floor and bend one knee, so that this side of the pelvis drops), how do they feel side to side?
Do you notice a difference? Is one more natural, the other one a bit more hard going? Maybe differences in ranges? You might have just found something interesting in terms of adducting or abducting each hip!
When you hike one side, do you notice that the whole leg rocks to the outside with it? Remember that we are interested in 'clean' hip motion, not just pelvis-and-leg-together motion.
Do you notice that there is a difference in weight distribution? For example, it often happens that, no matter which side drops, the weight always ends up in the same leg. With clean hip motion this should not really be the case...
What can the left and right hip do in terms of adduction and abduction? If you have problems with your adductors or the outside of your hip this is extremely relevant.
3. Transverse plane hip motion

For this one we will think "groin" because sometimes this is difficult for people to visualise. When you turn your pelvis to your left, you would be turning "into" the left groin and close it, whilst you would be turning "away from" the right groin. Turning towards that groin gives us hip internal rotation, turning away opens the space and gives us hip external rotation.
Turn your pelvis left and right...
Do you notice that one is easy, one restricted, maybe painful? According to the image, what does that tell you about your ability to internally or externally rotate each hip?
Do you feel that you are turning "into" and "away from" one leg, or is there actually no distinction between the pelvis motion and the leg?
Piriformis problems, IT Band problems, groin problems? Why might you have those based on your findings? What can and can't that hip do?
Moving on a spectrum - again
You might have found differences in these tests. Maybe you have more problems in one plane of motion than another. Maybe you noticed that there seems to be a problem with one hip but not so much with the other. Maybe you have found that one of these tests creates your problems! That would be great, because it would really tell you what specifically we want to to restore.
Either way, it hopefully gave you a little insight into why a hip might be complaining.
For example, maybe it was difficult to turn to the left and you had some kind of discomfort or a lack of range of motion. Remember when we talked about our movement spectrum here?

What this might tell you is that you are biased towards the right because the left is inaccessible. This would mean that your perception is probably biased towards a right hip that is internally rotated (closed)...a pinching right hip might be the outcome of that. Or maybe even sciatica as the backside of the hip would be under a lot of tension.
Connecting the dots & restoring your spectrum
There are many possible reasons for differences in these motions. It is very common that some of the reasons are in the the feet and legs. In the frontal plane paragraph I talked about weight distribution. If this was you, no matter which side drops and the weight stays in the same leg in both cases, the question might be: why does your body not want to put weight into that other leg? And from there, you can hopefully begin to see what the hip itself might not be the problem at all. It might just be stuck where it is due to that inability to move to the other leg...
Mapping the hip to the upper body
For now, we will continue with our map from before though because very often this can also really clear things up (and going into the legs now would confuse things). In the map article I described how we want to re-organise the shapes, so that we are not on the gas and the brake pedal at the same time (told you to read it :))
Difficulty rotating the pelvis one way
So let's stick with one of the examples above: We have difficulty turning the pelvis to the left, therefore to internally rotate the left hip and externally rotate the right hip.
Based on our map, we would be interested in whether the rib cage/spine can turn the other way: to the right.
Can it? Or is that difficult, too? Teach the spine to turn right, that leaves the pelvis relatively left. The question is: Why might you be unable to turn that spine right?
Difficulty anteriorly tilting

Another example: maybe you found that it was painful in the lower back to anteriorly tilt the pelvis. Which other shape in the upper body have you learned about that relates to that anterior tilt?
(*thinking pause*)
- It was the lifting of the chest (extension of the thoracic spine). What if your hip cannot go through this motion because the upper body is creating the other? How can you find out? By exploring the combinations in your body.
Difficulty posteriorly tilting

This is the opposite of the anterior tilting example. Even though many people think that they have a "slouched posture", it is actually really difficult to truly flex the spine and to open the back of the rib cage. The outcome here is that the pelvis is not really posteriorly tilting, and instead the knees commonly push forwards with a bend. Get movement into that spine and see what happens!
Or we keep it really simple!
Maybe that hip itself just really needs to learn how to move again. Lots of sitting can eliminate a lot of hip motion so let's get it back in this case. The tests themselves may become the exercise in this case, but with a clear focus on what should actually happen - not by allowing all those compensations again. Be clear and be honest about your movement. If it hurts, it's not quite right :)
Let me know what you find!
Comments